Flanders Quality Model (FlaQuM): Building the Invisible Engine of Quality in Healthcare
The Flanders Quality Model, FlaQuM, is a evidence based quality model that supports hospitals in developing a sustainable quality management system. Download here the new manuscript FlaQuM in a nutshell, a 3 pager explaining the model.
Listen also to the new Podcast on FlaQuM via Spotify https://ap.lc/fEdUI
A new approach to quality management that goes beyond checklists and inspections
Why do hospitals that follow the same standards still achieve very different results? According to Professor Kris Vanhaecht (KU Leuven), academic lead of Flanders Quality Model, the answer lies in something rarely addressed by traditional quality systems: the invisible engine inside every healthcare organization. The Flanders Quality Model, or FlaQuM, was designed to understand and strengthen that engine.
Towards a living system
“Many quality systems focus on compliance. Protocols are followed, inspections are passed, and certificates are framed on the wall. Yet performance still varies widely” says Professor Dirk De Ridder. FlaQuM starts from a different premise: quality is not a checklist, it is a living system embedded in culture, teamwork, leadership, and learning.
Developed as a co-creation between KU Leuven researchers and more than 20 Flemish hospitals, FlaQuM is a research-based consortium, under the daily coordination of Charlotte Van der Auwera, that helps organizations build quality management systems that work in daily practice, not just on paper. The mission is to support hospitals in developing a shared vision of quality, translating that vision into action, and strengthening their capacity to learn and innovate together.
A broader vision of quality
FlaQuM defines quality as multidimensional, multistakeholder, and multilevel. Quality includes not only safety and clinical outcomes, but also dignity, respect, and kindness. It is created with patients, families, professionals, and organizations. And it exists at every level, from bedside care to the boardroom. In this view, quality is not a moment, it is a way of working and thinking, every hour of every day.
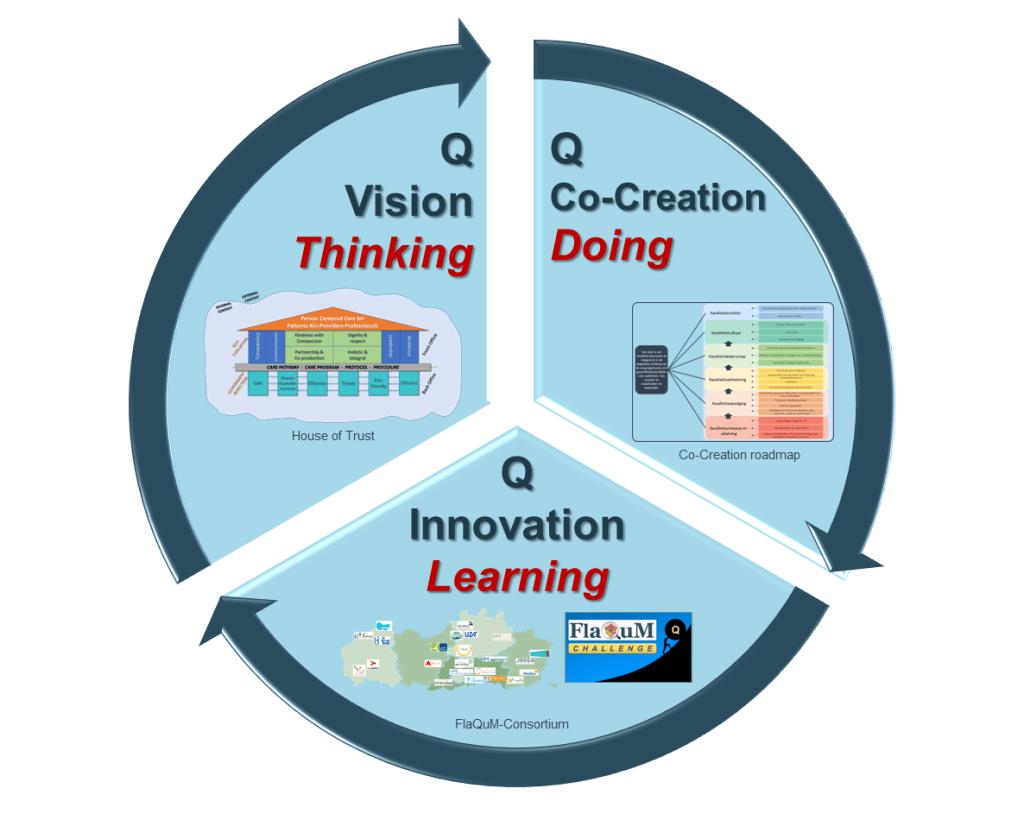
This perspective connects with the idea of Quality 1.0, 2.0, and 3.0 as previously internationally published by Lachman, Batalden & Vanhaecht in 2021. Quality 1.0 is the foundation: laws, standards, guidelines, and inspections. Quality 2.0 focuses on reliability, ensuring systems work every day through robust processes and indicators. Quality 3.0, the most advanced level, is about co-producing health with professionals, patients, and families, making quality sustainable because it is shared. FlaQuM aims to help hospitals integrate all three layers into one coherent quality management system, built around three core pillars: Think, Do, and Learn
- Thinking based on a quality vision model;
- Doing by focusing on the implementation of the co-creation roadmap;
- Learning from innovation and social capital in interhospital collaboratives.
Think is about building a shared vision. FlaQuM uses the “House of Trust” model, which distinguishes between back-office dimensions such as efficiency and sustainability, and front-office dimensions such as empathy, dignity, communication, and leadership. Importantly, these perspectives are measured not only among patients but also among healthcare professionals, recognizing that high-quality patient care depends on a healthy and respectful work environment.
Do focuses on turning vision into action through co-creation. The FlaQuM Roadmap, based on doctoral research by Dr. Fien Claessens, describes six drivers, 19 building blocks, and 52 concrete core processes for quality management. Hospitals assess themselves using a Maturity Matrix and decide their own ambitions for improvement, while working within a shared evidence-based framework.
Learn is about continuous improvement and innovation. Participating organizations form a learning community where they share successes and failures, benchmark data and challenge each other. Through initiatives such as the FlaQuM Peer Challenge, hospitals visit each other, discuss maturity scores and survey results, and set priorities for the coming years. A multidisciplinary team of researchers and management advisors from KU Leuven is supporting this social capital network and learning eco-system (see picture).
Understanding variation
To better understand why quality differs between organizations, the FlaQuM research & support team (see picture) has launched a large research effort across 30 Belgian hospitals: the FlaQuM Triangle Study. It examines organizational context, system maturity, team dynamics such as psychological safety and team collaboration and we include the perspectives of all stakeholders . We support the hospitals in performing a FlaQuM multi-scan. Based on that scan, hospitals receive feedback reports to help them interpret their own data and improve their quality of care. Feedback is provided to understand the variation between the teams in one organisation and between different organisations. Under the lead of Dr. Deborah Seys the feedback is delivered in clear visual reports that support managers and clinicians in understanding their as-is situation and motivates them in defining clear ambitions. Later, the results of this multicenter benchmarking will be linked to outcomes like patient safety, mortality, operational capacity and financial performance. The overall learning points will be translated into pragmatic improvement projects. The goal of the FlaQuM Triangle Study is not just measurement and research, but actionable learning based on sound methods from PhD’s by Dr. Astrid Van Wilder, Dr. Eva Marie Castro, Dr. Jonas Brouwers and PhD Candidates Matthias Gils, Alexander Wytinck and Mathieu Louiset.

A growing international movement
FlaQuM hospitals share a clear ambition: by 2028, each participating organization aims to reach a baseline level on all 52 core processes of the Maturity Matrix. The peer review approach is being further professionalized. “We are also developing new training programs to prepare ambassadors who can embed the FlaQuM philosophy more deeply in their organizations”, says Jolien Palmaerts, the FlaQuM training officer. An international advisory board, under the lead of Dr. Peter Lachman, is mentoring and coaching the academic team at KU Leuven, as new partnerships are emerging beyond Flanders, including in countries such as the Netherlands, Canada, Norway, and Australia. To manage and guide the FlaQuM team and consortium, FlaQuM is nowadays a business division of KU Leuven Research & Development (LRD), the university knowledge and technology transfer office. The operational, legal and business support by LRD makes sure that FlaQuM builds a world ready for tomorrow, based on today’s excellent research performed in close collaboration with organisations from the FlaQuM eco-system.

Members of the International Advisory Board: Dominique Allwood Pedro Delgado M. Rashad Massoud, MD, MPH, FACP Albert Wu Ian Leistikow Helen Bevan Goran Henriks Jens Winther Jensen Massimiliano Panella don goldmann Christina Krause
International validation of FlaQuM
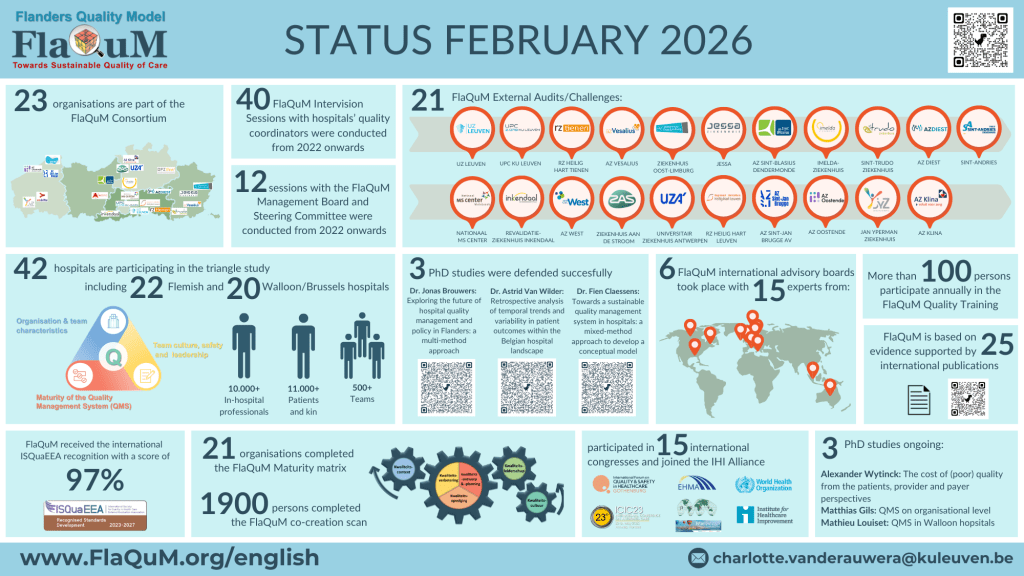
Since 2023, the FlaQuM model is validated by international experts and received the ISQuaEEA-recognition with a score of 97%. After a self-assessment, the components of the submitted system are screened by international experts and advised on where the system can make additional efforts in the next years.

Status February 2026
An invitation to quality leaders
For quality managers searching for the next level of quality management, FlaQuM offers more than tools. It offers a community, a shared language, and an evidence-based way to build the internal engine that drives sustainable quality. Each hospital builds its own system, tailored to its context, but within a common framework that supports learning across organizations.
“In a world where healthcare systems are under constant pressure, FlaQuM shows that lasting quality is not enforced from outside, it is cultivated from within. Our strategy is to do this in continuous collaboration with peer organisations worldwide and all quality management models used in healthcare should be based on sound academic research. That is what patients, their relatives and our multidisciplinary teams expect and deserve. That may be the most powerful quality strategy of all” concludes Prof. Kris Vanhaecht.
FOR MORE INFORMATION: Contact our FlaQuM project manager Charlotte Van der Auwera Listen to the Podcast on FlaQuM via Spotify https://ap.lc/fEdUI
